
For women navigating Polycystic Ovary Syndrome (PCOS), the struggle with weight management is rarely a matter of discipline or diet. It is a complex endocrine cascade driven primarily by severe, underlying insulin resistance. As the search for effective, sustainable treatments has intensified, the use of berberine for pcos weight loss has emerged as one of the most promising and heavily researched interventions in modern metabolic medicine.
But how effective is this plant-derived alkaloid compared to standard pharmaceuticals like Metformin? Can it actually lower androgens, restore ovulatory function, and drive fat loss without destroying your digestive system?
In this comprehensive clinical guide, we will analyze the peer-reviewed data on how berberine alters the hormonal landscape of PCOS. We will compare its efficacy directly against Metformin, expose the gastrointestinal crisis ("Berberine Belly") that causes so many women to quit the treatment early, and explain why transdermal delivery systems have become the clinical standard for PCOS management.
The Superior Berberine Delivery Method
Women with PCOS already suffer from gut inflammation. Bypass the stomach cramps entirely with medical-grade transdermal patches.
Shop Transdermal BerberineThe Biological Root of PCOS Weight Gain
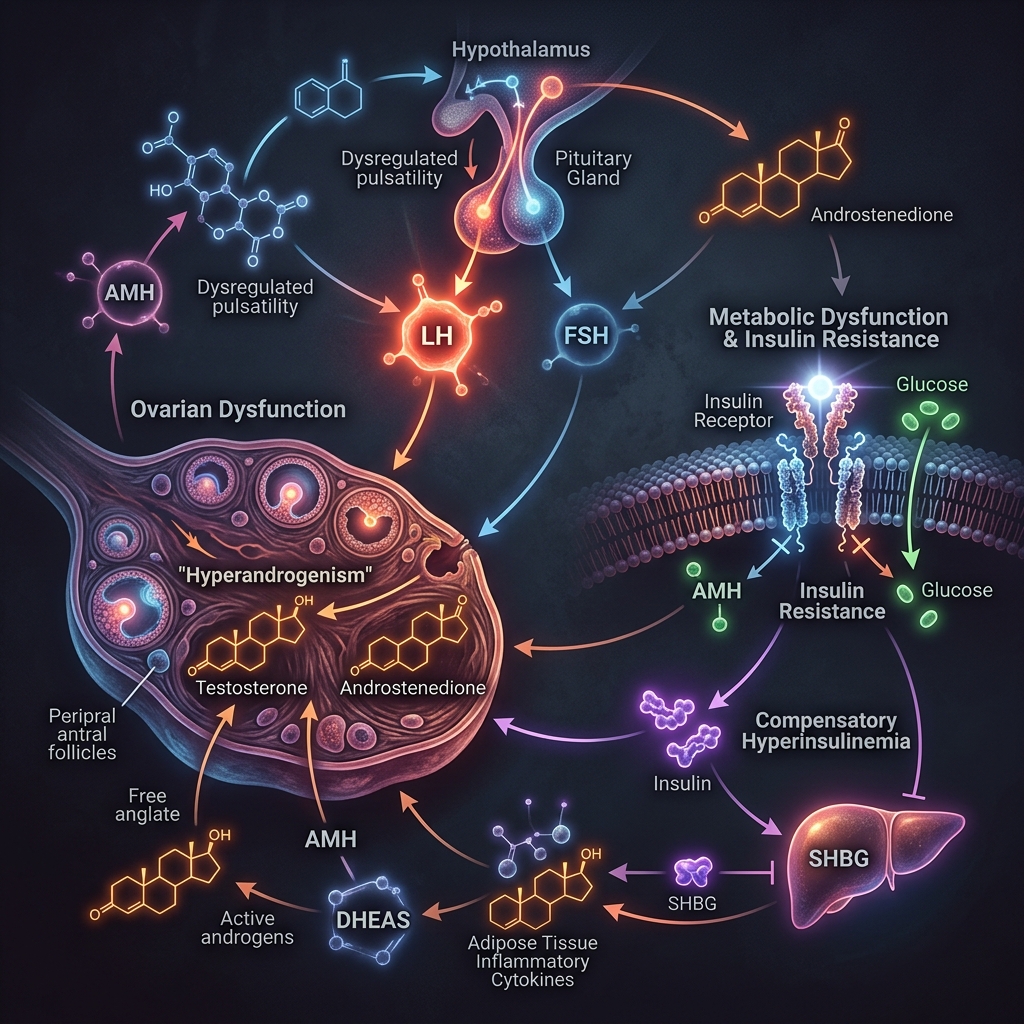
To understand why berberine is so effective, we must first understand the architecture of PCOS. While it is classified as a reproductive disorder, PCOS is fundamentally a metabolic condition. Up to 70-80% of women with PCOS suffer from insulin resistance, regardless of whether they are lean or overweight.
The Insulin-Androgen Feedback Loop
When cells become resistant to insulin, the pancreas pumps out massive amounts of insulin to force blood sugar levels down. This chronic state of hyperinsulinemia (high blood insulin) creates a devastating feedback loop in the female body:
- Ovarian Overstimulation: High insulin levels directly stimulate the theca cells in the ovaries to overproduce androgens (like testosterone).
- SHBG Suppression: High insulin signals the liver to drastically reduce the production of Sex Hormone-Binding Globulin (SHBG). SHBG normally binds to testosterone and renders it inactive. Without it, free testosterone runs rampant in the bloodstream, causing hirsutism (facial hair), acne, and hair loss.
- Fat Storage Lock: As we explored in our breakdown of insulin resistance, high insulin biologically disables hormone-sensitive lipase (HSL), making it physically impossible to burn stored visceral fat, no matter how hard you diet.
How Berberine Intervenes in PCOS
Berberine does not directly manipulate sex hormones. Instead, it strikes at the metabolic root of the condition by activating AMP-activated protein kinase (AMPK), the master switch of cellular energy.
1. Sensitizing the Receptors
By activating AMPK, berberine upregulates the expression of insulin receptors on the surface of your cells. It allows your body to clear glucose from the bloodstream using a fraction of the insulin it required previously. As insulin levels drop, the ovaries stop being hyper-stimulated, and testosterone production plummets.
2. Restoring SHBG Levels
Clinical trials show that berberine significantly increases the liver's production of SHBG. This newly produced SHBG acts as a sponge, soaking up the excess free testosterone in the blood and mitigating the physical symptoms of hyperandrogenism (acne, hair growth).
3. Unlocking Fat Oxidation
With insulin levels finally normalized, the biological "lock" on fat storage is removed. The body can once again access visceral fat stores for energy, facilitating sustainable, consistent weight loss that is almost impossible to achieve when hyperinsulinemic.
The Clinical Data: Berberine vs Metformin
For decades, the standard first-line pharmaceutical treatment for PCOS-induced insulin resistance has been Metformin. However, a growing body of robust clinical evidence suggests that berberine is not only a viable alternative but, in some metrics, superior.
| Clinical Marker | Metformin (1500mg/day) | Berberine (1500mg/day) |
|---|---|---|
| Insulin Resistance (HOMA-IR) | Significant Reduction | Significant Reduction (Equivalent to Metformin) |
| Lipid Profile (Total Cholesterol & LDL) | Mild to Moderate Improvement | Superior Improvement (Significant drops in Triglycerides and LDL) |
| Total Testosterone Reduction | Effective Reduction | Effective Reduction (Equivalent to Metformin) |
| SHBG Increase | Moderate Increase | Superior Increase |
| Pregnancy/Ovulation Rates | Highly Effective (First-line for fertility) | Highly Effective (Often improves live birth rates in IVF protocols) |
In a landmark clinical study (Wei et al., 2012) comparing berberine to metformin in women with PCOS, researchers found that berberine yielded identical results to metformin in reducing insulin resistance and increasing ovulation rates. However, berberine dramatically outperformed metformin in improving lipid profiles (lowering triglycerides and total cholesterol) and increasing SHBG.
Content Gap: The Unspoken Nightmare of "Berberine Belly" in PCOS
If the data is so incredible, why isn't every woman with PCOS successfully losing weight on berberine? Most major health blogs and fertility websites fail to mention the critical flaw in standard berberine therapy: oral bioavailability and gastrointestinal destruction.
Women with PCOS are highly predisposed to gut dysbiosis, chronic low-grade inflammation, and Irritable Bowel Syndrome (IBS). Standard oral berberine has an absolute bioavailability of less than 1%. To achieve the metabolic effects seen in the clinical trials, you must ingest massive oral doses (500mg, three times a day).
Because it is a highly potent antimicrobial, throwing 1,500mg of raw berberine powder into an already compromised PCOS gut is often a disaster. Up to 34% of users experience severe gastrointestinal adverse events—cramping, explosive diarrhea, and nausea—often referred to as "Berberine Belly." Many women are forced to abandon the therapy before they ever see the metabolic benefits.
The Transdermal Solution
In 2026, forcing a compromised gut to process raw alkaloids is outdated medicine. As we detailed in our Berberine vs Ozempic comparison guide, the clinical standard has shifted to transdermal delivery systems.
By utilizing medical-grade transdermal patches, berberine (and its highly bioavailable derivative, dihydroberberine) is absorbed directly through the skin barrier and into the microcirculation over a 24-hour period. This completely bypasses the gastrointestinal tract and avoids first-pass liver metabolism. The result? Steady, sustained AMPK activation with absolutely zero stomach cramps, zero diarrhea, and no gut flora destruction.
Protect Your Gut Microbiome
Achieve clinical-grade AMPK activation without the gastrointestinal distress of oral pills. Discover transdermal berberine.
View Transdermal OptionsWhat if Berberine Isn't Enough? (The GLP-1 Escalation)
While berberine is a powerful tool, it is not a miracle drug. If a patient has severe, long-standing PCOS with a BMI over 35 and deeply entrenched insulin resistance, the gentle AMPK activation of transdermal berberine may not be enough to break the cycle.
In these cases, clinicians frequently escalate to GLP-1 receptor agonists, such as Semaglutide or Tirzepatide. These medications force the pancreas to correct insulin secretion and exert massive, CNS-level appetite suppression, often resulting in 15-20% total body weight loss. This rapid reduction in visceral fat acts as a hard reset for the endocrine system, frequently restoring regular menstrual cycles and ovulation within months.
Need a Stronger Intervention?
If natural options have failed, see if you qualify for clinician-guided GLP-1 therapy starting at $146/mo.
Start Medical AssessmentFrequently Asked Questions (FAQ)
How long does it take for berberine to work for PCOS weight loss?
Metabolic recalibration takes time. While insulin sensitivity begins improving within days, visible changes in weight, reductions in facial hair, and the return of ovulatory cycles typically require 8 to 12 weeks of consistent, daily administration.
Can I take berberine if I am trying to get pregnant?
Berberine is highly effective at restoring ovulation and is often used in the preconception phase to improve egg quality. However, it is strictly contraindicated during actual pregnancy and breastfeeding. You must stop taking berberine the moment you receive a positive pregnancy test.
Can I take berberine and Metformin together?
Because both compounds activate AMPK and lower blood sugar, combining them can lead to hypoglycemia (dangerously low blood sugar) and severe gastrointestinal distress. You should not combine them without strict, direct supervision from your endocrinologist.
Will berberine cure my PCOS?
PCOS is a genetic and epigenetic condition that cannot be "cured." It can, however, be aggressively managed and put into remission. By utilizing transdermal berberine to control insulin resistance, you can eliminate the symptoms of the syndrome and maintain a healthy metabolic profile long-term.
Ready to Take Control of Your PCOS?
Whether you want the targeted support of transdermal berberine or the clinical power of compounded GLP-1s, we provide the highest quality metabolic treatments available.
Academic References & Clinical Citations
- Wei, W., Zhao, H., Wang, A., Sui, M., Liang, K., Deng, H., Ma, Y., Zhang, Y., Zhang, H., & Guan, Y. (2012). A clinical study on the short-term effect of berberine in comparison to metformin on the metabolic characteristics of women with polycystic ovary syndrome. European Journal of Endocrinology, 166(1), 99–105. https://pubmed.ncbi.nlm.nih.gov/22019891/
- Zhao, J. V., Yeung, W. F., Chan, Y. H., Vackova, D., Leung, J. Y. Y., Jiang, L., Lee, V. C. Y., Li, T. C., & Schooling, C. M. (2021). Effect of berberine on polycystic ovary syndrome: a systematic review and meta-analysis. Gynecological Endocrinology, 37(11), 966–972. https://pubmed.ncbi.nlm.nih.gov/34145942/
- Rondanelli, M., Infantino, V., Riva, A., Petrangolini, G., Faliva, M. A., Peroni, G., Naso, M., Nichetti, M., Spadaccini, D., Gasparri, C., & Perna, S. (2020). Polycystic ovary syndrome management: a review of the possible amazing role of berberine. Archives of Gynecology and Obstetrics, 301(1), 53–60. https://pubmed.ncbi.nlm.nih.gov/32060683/