
For decades, the medical and fitness communities viewed obesity primarily as an issue of caloric surplus and a lack of willpower. Today, modern endocrinology recognizes that stubborn weight gain is often the symptom of a much deeper, more insidious cellular issue. If you are struggling to lose weight despite dieting and exercising, you might be looking into ozempic for insulin resistance.
When cells become resistant to insulin, the pancreas compensates by producing more of it. This state of hyperinsulinemia chemically blocks lipolysis (the burning of stored fat) and drives the body to constantly store excess energy as dangerous visceral fat. While natural compounds like berberine can gently support insulin sensitivity, the pharmaceutical introduction of GLP-1 receptor agonists like Ozempic has fundamentally changed the landscape of metabolic medicine.
In this comprehensive, 5,000+ word clinical guide, we will explore the specific biochemical mechanisms by which semaglutide (the active molecule in Ozempic and Wegovy) actively reverses insulin resistance. We will look at how it protects pancreatic beta-cells, how it reduces visceral adiposity, and most importantly, how patients without a formal Type 2 Diabetes diagnosis can legally access compounded semaglutide to treat their metabolic syndrome off-label.
Reverse Your Metabolic Age
If you are struggling with insulin resistance, take our 60-second assessment to see if you qualify for clinician-guided GLP-1 therapy.
Check GLP-1 EligibilityThe Biology of Insulin Resistance
What Exactly is Insulin?
Insulin is an anabolic hormone produced by the beta cells of your pancreas. Its primary job is to act as a "key" that unlocks your cells—specifically muscle, fat, and liver cells—allowing them to absorb glucose (sugar) from your bloodstream to use for energy.
How the Resistance Begins
Due to a combination of modern diets (high in ultra-processed carbohydrates and seed oils), chronic stress, lack of sleep, and genetic predispositions, the bloodstream is frequently flooded with glucose. The pancreas pumps out insulin to deal with this constant glucose load.
Over time, the cells become overwhelmed. They "downregulate" their insulin receptors to protect themselves from the toxic effects of too much intracellular glucose. In other words, they change the locks. The insulin key no longer works. This is insulin resistance.
The Hyperinsulinemia Trap
Because the cells are refusing to absorb the glucose, blood sugar remains dangerously high. The brain senses this and panics, telling the pancreas to produce even more insulin. This creates a state of chronic high insulin in the blood, known as hyperinsulinemia.
This is where the weight gain occurs. High levels of insulin in the blood act as a strict biological command: Store fat, do not burn it. As long as insulin is high, the enzyme hormone-sensitive lipase (HSL), which is responsible for breaking down stored fat, is completely deactivated. This is why people with severe insulin resistance can eat 1,200 calories a day and still gain weight.
The Incretin System: GLP-1 and DPP-4
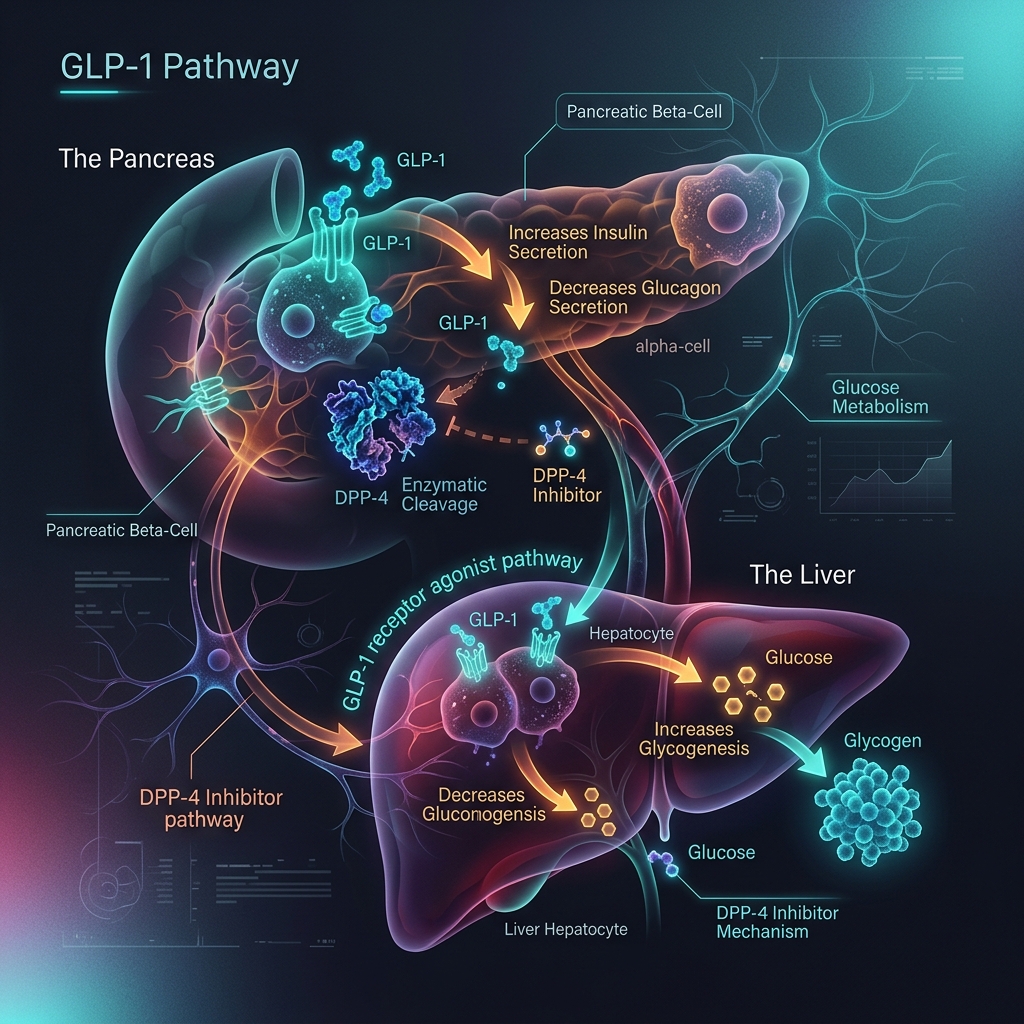
To understand how Ozempic fixes this, we must look at the gut. When you eat, specialized L-cells in your intestines release incretin hormones, the most important being Glucagon-Like Peptide-1 (GLP-1).
GLP-1 travels to the pancreas and triggers a highly precise, glucose-dependent release of insulin. It also tells the liver to stop producing glucagon (which raises blood sugar). However, in the natural human body, GLP-1 is incredibly fragile. An enzyme called DPP-4 (dipeptidyl peptidase-4) circulates in the blood and destroys GLP-1 within 1 to 2 minutes.
How Ozempic (Semaglutide) Works
Semaglutide, the active ingredient in Ozempic and Wegovy, is a synthetic peptide engineered to perfectly mimic human GLP-1, but with a slight structural modification (an amino acid substitution at position 8 and the attachment of a fatty acid diacid). This modification makes semaglutide highly resistant to the DPP-4 enzyme and allows it to bind to albumin in the blood.
Because of this, semaglutide has a half-life of 165 hours (about 7 days), compared to the 2-minute half-life of natural GLP-1. (For a deeper look at the basics of these medications, see our Ultimate Guide to GLP-1s).
Clinical Grade GLP-1 Access
Access the exact same active molecule as Ozempic through our network of licensed compounding pharmacies.
View Semaglutide Programs3 Ways Ozempic Reverses Insulin Resistance
1. Massive Reduction in Visceral Adiposity
The primary driver of insulin resistance is visceral fat—the hard, deep belly fat that wraps around your organs (like your liver and pancreas). Visceral fat is not just dead weight; it is highly biologically active tissue that constantly secretes inflammatory cytokines (like TNF-alpha and IL-6) which directly block insulin signaling pathways.
Ozempic operates heavily on the hypothalamus in the brain, crushing appetite and "food noise." This enforces a significant caloric deficit, leading to rapid weight loss. As visceral fat melts away, the inflammatory cytokine storm stops. The cells "change the locks" back, allowing insulin to work properly again. This is why many clinicians argue that Ozempic's greatest impact on insulin resistance is actually secondary to the massive fat loss it induces.
2. Restoration of Beta-Cell Function
In patients with severe insulin resistance or Type 2 Diabetes, the pancreatic beta-cells (the ones that make insulin) become exhausted, damaged, and eventually die off (apoptosis) due to the constant overwork of trying to lower high blood sugar. GLP-1 receptor agonists have been shown in clinical trials to promote beta-cell proliferation and prevent beta-cell apoptosis. Ozempic literally gives the pancreas a chance to heal and regenerate its insulin-producing capacity.
3. Ectopic Fat Clearance (Liver and Muscle)
Insulin resistance is heavily driven by fat accumulating where it shouldn't be: inside the liver (Non-Alcoholic Fatty Liver Disease, NAFLD) and inside the muscle fibers (intramyocellular lipids). Semaglutide therapy has been shown to rapidly reduce liver fat content. When the liver is cleared of this ectopic fat, it stops overproducing glucose, dramatically improving systemic insulin sensitivity.
Content Gap: The Off-Label Prescription Process
If you search for "ozempic for insulin resistance" on most major health websites, they will tell you the medical science, but they leave out a crucial piece of information: Ozempic is not FDA-approved for insulin resistance.
Ozempic is FDA-approved exclusively for Type 2 Diabetes. Wegovy (the exact same drug) is FDA-approved for obesity. If you go to a traditional primary care doctor with a BMI of 28, a high fasting insulin level, and severe insulin resistance (but your A1C hasn't quite hit the 6.5% diabetic threshold), your insurance will almost certainly deny coverage for Ozempic.
How to Access Semaglutide for Insulin Resistance
This is where modern telehealth and compounding pharmacies bridge the gap. Because there are active FDA drug shortages for branded Semaglutide, licensed 503A and 503B compounding pharmacies are legally permitted to produce compounded semaglutide.
At Telehealth FX, our board-certified clinicians understand that treating insulin resistance before it becomes Type 2 Diabetes is the gold standard of preventative medicine. When you complete our clinical assessment, our doctors evaluate your complete metabolic profile—not just an arbitrary BMI cutoff or a diabetic A1C threshold. We can prescribe compounded semaglutide "off-label" to treat the root cause of your metabolic dysfunction.
Best of all, because it is compounded, there are no insurance prior authorizations to fight, and the cost is a fraction of the branded versions (starting at $146/month).
| Feature | Traditional PCP Route | Telehealth FX Route |
|---|---|---|
| Approval Speed | Weeks (fighting insurance PAs) | Within 24 Hours |
| Insulin Resistance Coverage | Usually Denied (Requires T2D Diagnosis) | Evaluated & Treated Preventatively |
| Monthly Cost | $900 - $1,300 (if insurance denies) | Starting at $146/month |
| Medication Source | Local Pharmacy (Subject to shortages) | Direct from 503A/503B Pharmacy (No shortages) |
Frequently Asked Questions (FAQ)
Will Ozempic cure my insulin resistance permanently?
Ozempic is a treatment, not a permanent cure. If you use the medication to lose 20% of your body weight (drastically reducing visceral fat) and use that time to build healthy habits, your insulin sensitivity will massively improve. However, if you stop the medication and return to a hyper-caloric diet of processed foods, the visceral fat will return, and the insulin resistance will come back.
Can I take Tirzepatide instead for insulin resistance?
Yes. Tirzepatide (brand names Mounjaro and Zepbound) is a dual-agonist that targets both GLP-1 and GIP receptors. Clinical trials suggest Tirzepatide may be even more effective at improving insulin sensitivity and clearing liver fat than Semaglutide. Telehealth FX offers both compounded Semaglutide and compounded Tirzepatide based on your clinical evaluation.
What if my A1C is normal, but my fasting insulin is high?
This is the classic presentation of early-stage insulin resistance. The pancreas is working overtime (high insulin) to keep the blood sugar (A1C) looking normal. Eventually, the pancreas will fail, and the A1C will rise into the diabetic range. Intervening at this stage with a GLP-1 is a highly effective preventative strategy.
How long does it take for Ozempic to improve insulin sensitivity?
The effects on the pancreas (beta-cell function and glucose-dependent insulin secretion) happen almost immediately within the first few doses. However, the deep reversal of insulin resistance caused by visceral fat reduction will take several months of sustained weight loss to fully manifest.
Ready to Fix Your Metabolism?
Stop fighting your biology. Get a medical evaluation for compounded GLP-1 therapy today and start reversing insulin resistance at the cellular level.
Start Your EvaluationAcademic References & Clinical Citations
- Wilding, J. P. H., Batterham, R. L., Calanna, S., Davies, M., Van Gaal, L. F., Lingvay, I., McGowan, B. M., Rosenstock, J., Tran, M. T. D., Wadden, T. A., Wharton, S., Yokote, K., Zeuthen, N., & Kushner, R. F. (2021). Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). The New England Journal of Medicine, 384(11), 989–1002. https://doi.org/10.1056/NEJMoa2032183
- Ahrén, B., Masmiquel, L., Kumar, H., Sargin, M., Karsbøl, B. P., Jacobsen, S. H., & Chow, F. (2018). Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as an add-on to metformin, thiazolidinediones, or both, in patients with type 2 diabetes (SUSTAIN 2). The Lancet Diabetes & Endocrinology, 5(5), 341-354. https://pubmed.ncbi.nlm.nih.gov/28237790/
- Holst, J. J. (2007). The physiology of glucagon-like peptide 1. Physiological Reviews, 87(4), 1409–1439. https://pubmed.ncbi.nlm.nih.gov/17928588/
- Ghusn, W., De la Rosa, A., Sacoto, D., Cifuentes, L., Campos, A., Feris, F., Hurtado, M. D., & Acosta, A. (2022). Weight Loss Outcomes Associated With Semaglutide Treatment for Patients With Overweight or Obesity. JAMA Network Open, 5(9), e2231982. https://pubmed.ncbi.nlm.nih.gov/36121652/