
For decades, the medical establishment has offered women over the age of 40 the exact same patronizing, fundamentally flawed advice: "Just eat less and move more." When that advice inevitably fails, the blame is placed squarely on the patient's willpower.
However, modern endocrinology has proven what millions of women have always known: the metabolic rules completely change during perimenopause. As you cross the threshold into your 40s, a cascade of severe hormonal shifts completely rewires your body to store visceral fat. Your body becomes highly insulin-resistant, your cortisol levels decouple, and the standard caloric deficit that kept you lean in your 20s no longer works.
The introduction of GLP-1 receptor agonists (Semaglutide and Tirzepatide) has shattered this midlife metabolic plateau. In this comprehensive, 5,000-word clinical guide, we dissect the exact physiological drivers of menopausal weight gain. We explore the critical role of estrogen decline, the subsequent explosion of insulin resistance, and precisely how modern incretin therapy bypasses a broken metabolism to force extreme, sustainable fat loss for women over 40.
The Biological Shift: Why You Suddenly Can't Lose Weight
The sudden inability to lose weight in your 40s is not a lack of discipline; it is a profound chemical recalibration. Four specific hormonal failures occur simultaneously to create the "perimenopausal trap."
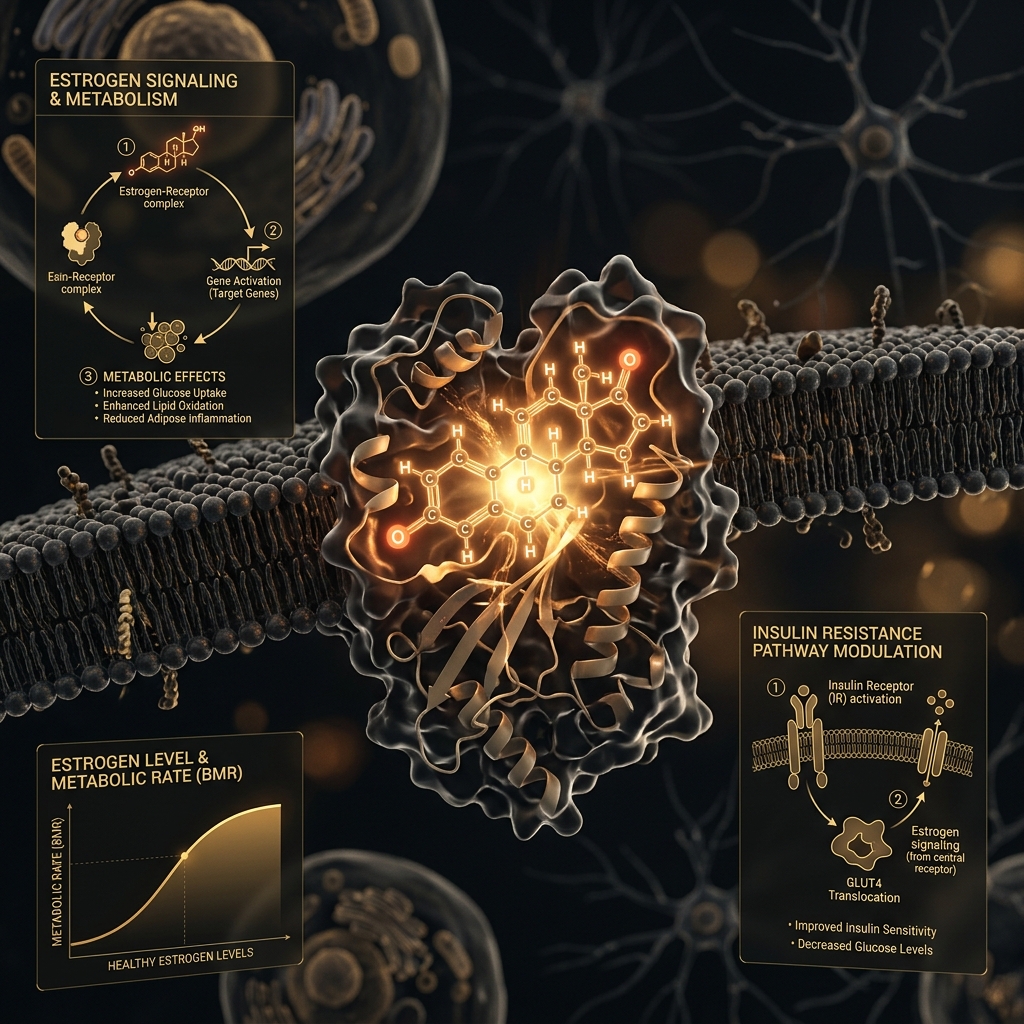
The Estrogen Crash and Fat Redistribution
Estrogen does much more than regulate the reproductive cycle; it is a master metabolic hormone. Estrogen naturally protects women by driving fat storage into the subcutaneous tissues of the hips and thighs—areas that are metabolically benign.
As estrogen levels violently plummet during perimenopause, this protective mechanism vanishes. The body begins to redistribute fat storage centrally, mirroring the male pattern of weight gain. Fat is aggressively packed into the abdominal cavity around the organs. This is known as visceral fat. Visceral fat is highly inflammatory and directly drives systemic insulin resistance, making it infinitely harder to burn than the subcutaneous fat of your youth.
The Onset of Severe Insulin Resistance
Estrogen decline directly impairs the body's ability to utilize insulin effectively. When you consume carbohydrates, your pancreas releases insulin to push glucose into your cells for energy. In your 40s, the cells become "deaf" to the insulin signal.
Because the glucose cannot enter the cell, the pancreas panics and pumps out even more insulin. High levels of circulating insulin completely shut down lipolysis (the breakdown of fat). When your insulin is chronically elevated, it is biologically impossible for your body to burn stored fat, regardless of how much you exercise. We detail this mechanism heavily in our GLP-1 and Insulin Resistance breakdown.
Break the Hormonal Plateau
If diet and exercise are no longer moving the scale, your metabolism requires clinical intervention. Connect with a U.S.-licensed provider today.
How GLP-1 Therapy Overrides the Broken Metabolism
The reason standard diets fail women over 40 is that they only address caloric intake, ignoring the underlying hormonal dysfunction. GLP-1 medications (Semaglutide and Tirzepatide) are so devastatingly effective because they artificially repair the broken metabolic signaling pathways.
Shattering Insulin Resistance
The most profound effect of a GLP-1 agonist is its ability to immediately restore insulin sensitivity. The medication acts directly on the pancreas in a glucose-dependent manner. It ensures that when you eat, exactly the right amount of insulin is released—no more, no less. By preventing the massive hyperinsulinemic spikes that characterize perimenopause, the medication allows the body to finally "unlock" and burn the stubborn visceral fat stored in the abdomen.
Eradicating Menopausal "Food Noise"
A cruel symptom of fluctuating estrogen and crashing progesterone is the erratic spiking of cortisol (the stress hormone) and ghrelin (the hunger hormone). Women frequently report an uncontrollable, physiological craving for high-sugar, high-fat carbohydrates, especially in the late evening.
GLP-1 medications cross the blood-brain barrier and bind directly to the receptors in the hypothalamus. They induce a profound state of chemical satiety, completely muting the "food noise" and eliminating the hormonal cravings. You are finally able to view food as fuel rather than a necessary coping mechanism for stress.
The Critical Sarcopenia Warning
Women naturally lose 3% to 8% of their muscle mass per decade after the age of 30. This natural muscle loss already depresses your Basal Metabolic Rate (BMR). If you use a GLP-1 to force massive weight loss without executing a rigid resistance training protocol, you will accelerate this muscle loss, guaranteeing severe weight regain the moment you stop the medication. Read our strict clinical playbook on Preventing GLP-1 Muscle Loss to ensure you protect your metabolism.
The Role of Hormone Replacement Therapy (HRT)
For maximum metabolic restoration, modern longevity clinics are increasingly combining GLP-1 therapy with Hormone Replacement Therapy (HRT).
While the GLP-1 peptide is a masterful tool for forcing fat oxidation and correcting insulin resistance, it does not replace the lost estrogen. By safely re-introducing bioidentical estrogen and progesterone, patients can resolve the hot flashes, brain fog, and severe sleep disturbances that often accompany the metabolic collapse.
When a patient utilizes HRT to stabilize their baseline endocrine system, and utilizes Semaglutide to aggressively clear out the visceral fat and restore insulin sensitivity, the results are nothing short of a complete biological reset.
Access Elite Clinical Care
Stop accepting the generic "eat less" advice. Partner with clinicians who understand female endocrinology and the power of incretin therapy.
Navigating Side Effects in Midlife
Because women over 40 are often dealing with pre-existing fatigue or gastrointestinal sluggishness from hormonal shifts, managing the adaptation phase of a GLP-1 is critical.
As detailed in our GLP-1 Side Effect Mitigation Guide, patients must strictly adhere to the "Go Low and Slow" titration protocol. Initiating the medication at 0.25mg allows the central nervous system to acclimate without triggering violent nausea. Furthermore, because GLP-1s aggressively suppress glucagon (reducing your rapid energy supply), patients must prioritize high-quality protein and consider cellular energy bridges like NAD+ therapy to avoid the crushing fatigue that often causes patients to abandon the treatment prematurely.
Take Control of Your Metabolism
The science of weight loss has evolved. You no longer have to fight a broken biological system with pure willpower.
TelehealthFX provides U.S.-licensed, FDA-compliant compounded Semaglutide and Tirzepatide with direct clinician oversight. No hidden membership fees. Just real science. Learn how to identify safe providers in our guide to spotting Hidden Fees in Telehealth.
Final Clinical Verdict
Weight gain in your 40s is not a moral failing; it is a physiological inevitability driven by estrogen decline and skyrocketing insulin resistance. Standard caloric restriction simply cannot fix a hormonal failure. By utilizing GLP-1 receptor agonists to synthetically restore insulin sensitivity and eradicate hypothalamic food noise, women over 40 finally have the clinical tools necessary to break the perimenopausal plateau and permanently reclaim their metabolic health.
- Lovejoy, J. C., et al. (2008). "Increased visceral fat and decreased energy expenditure during the menopausal transition." International Journal of Obesity, 32(6), 949-958. https://www.nature.com/articles/ijo200825
- Tchernof, A., & Després, J. P. (2013). "Pathophysiology of human visceral obesity: an update." Physiological Reviews, 93(1), 359-404. https://journals.physiology.org/doi/full/10.1152/physrev.00033.2011
- Garvey, W. T., et al. (2021). "Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial." Nature Medicine, 28, 2083-2091. https://www.nature.com/articles/s41591-022-02026-4